No está mal tirado, pero el problema es que para un uso continuado las cosas deben esterilizarse y no todo es esterilizable. Aunque la verdad es que las gafas que 3M y compañía fabrican, en diseño, no difieren mucho de las de natación . Se están usando mucho unas mascarillas que llevan visera incorporada. Funcionan muy bien. Son para usar y tirar, pero escasean mucho.
La verdad es que hay muchísimas opciones de protección, muchas de ellas además adaptadas a los tiempos de exposición de cada profesional. El problema es que escasean y que están llegando excesivamente tarde. No puede ser que viniendose lo que se estaba viendo en Italia te encuentres con UCIs y boxes de aislamiento que no tienen mascarillas con filtro o monos impermeables.
Pero bueno. Animo a todos que de esto se sale.
Pd: Y bajando el precio medio!!!
Mucho ánimo y no desesperes, intenta ser positivo y pensar en que todo pasará más pronto que tarde.
Yo conozco a varias personas que lo han tenido y ya están bien. Son 2 o 3 días de fiebre, fatiga y estar en la cama, pero nada más, ya está recuperadas. En palabras textuales suyas, como una gripe chunga…
Cuando haya pasado todo esto y si pasáis alguna vez, acordaros y parad a degustar sus deliciosas tostadas con aceite de oliva. PK. 110,200 A92 dirección Granada.
A veces conviene aislarse de todo el ruido mediático, tomar un poco de distancia y mantener una mente abierta. Independientemente de que el autor esté en lo cierto o no su planteamiento no deja de parecerme muy interesante. Copio todo el texto porque hay que crearse cuenta en el NY Times para poder acceder al artículo
Is Our Fight Against Coronavirus Worse Than the Disease?
We routinely differentiate between two kinds of military action: the inevitable carnage and collateral damage of diffuse hostilities, and the precision of a “surgical strike,” methodically targeted to the sources of our particular peril. The latter, when executed well, minimizes resources and unintended consequences alike.
As we battle the coronavirus pandemic, and heads of state declare that we are “at war” with this contagion, the same dichotomy applies. This can be open war, with all the fallout that portends, or it could be something more surgical. The United States and much of the world so far have gone in for the former. I write now with a sense of urgency to make sure we consider the surgical approach, while there is still time.
Outbreaks tend to be isolated when pathogens move through water or food, and of greater scope when they travel by widespread vectors like fleas, mosquitoes or the air itself. Like the coronavirus pandemic, the infamous flu pandemic of 1918 was caused by viral particles transmitted by coughing and sneezing. Pandemics occur when an entire population is vulnerable — that is, not immune — to a given pathogen capable of efficiently spreading itself.
Immunity occurs when our immune system has developed antibodies against a germ, either naturally or as a result of a vaccine, and is fully prepared should exposure recur. The immune system response is so robust that the invading germ is eradicated before symptomatic disease can develop.
Importantly, that robust immune response also prevents transmission. If a germ can’t secure its hold on your body, your body no longer serves as a vector to send it forward to the next potential host. This is true even if that next person is not yet immune. When enough of us represent such “dead ends” for viral transmission, spread through the population is blunted, and eventually terminated. This is called herd immunity.
What we know so far about the coronavirus makes it a unique case for the potential application of a “herd immunity” approach, a strategy viewed as a desirable side effect in the Netherlands, and briefly considered in the United Kingdom.
The data from South Korea, where tracking the coronavirus has been by far the best to date, indicate that as much as 99 percent of active cases in the general population are “mild” and do not require specific medical treatment. The small percentage of cases that do require such services are highly concentrated among those age 60 and older, and further so the older people are. Other things being equal, those over age 70 appear at three times the mortality risk as those age 60 to 69, and those over age 80 at nearly twice the mortality risk of those age 70 to 79.
These conclusions are corroborated by the data from Wuhan, China, which show a higher death rate, but an almost identical distribution. The higher death rate in China may be real, but is perhaps a result of less widespread testing. South Korea promptly, and uniquely, started testing the apparently healthy population at large, finding the mild and asymptomatic cases of Covid-19 other countries are overlooking. The experience of the Diamond Princess cruise ship, which houses a contained, older population, proves the point. The death rate among that insular and uniformly exposed population is roughly 1 percent.
We have, to date, fewer than 200 deaths from the coronavirus in the United States — a small data set from which to draw big conclusions. Still, it is entirely aligned with the data from other countries. The deaths have been mainly clustered among the elderly, those with significant chronic illnesses such as diabetes and heart disease, and those in both groups.
This is not true of infectious scourges such as influenza. The flu hits the elderly and chronically ill hard, too, but it also kills children. Trying to create herd immunity among those most likely to recover from infection while also isolating the young and the old is daunting, to say the least. How does one allow exposure and immunity to develop in parents, without exposing their young children?
The clustering of complications and death from Covid-19 among the elderly and chronically ill, but not children (there have been only very rare deaths in children), suggests that we could achieve the crucial goals of social distancing — saving lives and not overwhelming our medical system — by preferentially protecting the medically frail and those over age 60, and in particular those over 70 and 80, from exposure.
Why does this matter?
I am deeply concerned that the social, economic and public health consequences of this near total meltdown of normal life — schools and businesses closed, gatherings banned — will be long lasting and calamitous, possibly graver than the direct toll of the virus itself. The stock market will bounce back in time, but many businesses never will. The unemployment, impoverishment and despair likely to result will be public health scourges of the first order.
Worse, I fear our efforts will do little to contain the virus, because we have a resource-constrained, fragmented, perennially underfunded public health system. Distributing such limited resources so widely, so shallowly and so haphazardly is a formula for failure. How certain are you of the best ways to protect your most vulnerable loved ones? How readily can you get tested?
We have already failed to respond as decisively as China or South Korea, and lack the means to respond like Singapore. We are following in Italy’s wake, at risk of seeing our medical system overwhelmed twice: First when people rush to get tested for the coronavirus, and again when the especially vulnerable succumb to severe infection and require hospital beds.
Yes, in more and more places we are limiting gatherings uniformly, a tactic I call “horizontal interdiction” — when containment policies are applied to the entire population without consideration of their risk for severe infection.
But as the work force is laid off en masse (our family has one adult child home for that reason already), and colleges close (we have another two young adults back home for this reason), young people of indeterminate infectious status are being sent home to huddle with their families nationwide. And because we lack widespread testing, they may be carrying the virus and transmitting it to their 50-something parents, and 70- or 80-something grandparents. If there are any clear guidelines for behavior within families — what I call “vertical interdiction” — I have not seen them.
Such is the collateral damage of this diffuse form of warfare, aimed at “flattening” the epidemic curve generally rather than preferentially protecting the especially vulnerable. I believe we may be ineffectively fighting the contagion even as we are causing economic collapse.
There is another and much overlooked liability in this approach. If we succeed in slowing the spread of coronavirus from torrent to trickle, then when does the society-wide disruption end? When will it be safe for healthy children and younger teachers to return to school, much less older teachers and teachers with chronic illnesses? When will it be safe for the work force to repopulate the workplace, given that some are in the at-risk group for severe infection?
When would it be safe to visit loved ones in nursing homes or hospitals? When once again might grandparents pick up their grandchildren?
There are many possible answers, but the most likely one is: We just don’t know. We could wait until there’s an effective treatment, a vaccine or transmission rates fall to undetectable levels. But what if those are a year or more away? Then we suffer the full extent of societal disruption the virus might cause for all those months. The costs, not just in money, are staggering to contemplate.
So what is the alternative? Well, we could focus our resources on testing and protecting, in every way possible, all those people the data indicate are especially vulnerable to severe infection: the elderly, people with chronic diseases and the immunologically compromised. Those that test positive could be the first to receive the first approved antivirals. The majority, testing negative, could benefit from every resource we have to shield them from exposure.
To be sure, while mortality is highly concentrated in a select groups, it does not stop there. There are poignant, heart-rending tales of severe infection and death from Covid-19 in younger people for reasons we do not know. If we found over time that younger people were also especially vulnerable to the virus, we could expand the at-risk category and extend protections to them.
We have already identified many of the especially vulnerable. A detailed list of criteria could be generated by the Centers for Disease Control and Prevention, updated daily and circulated widely to health professionals and the public alike. The at-risk population is already subject to the protections of our current policies: social distancing, medical attention for fever or cough. But there are several major problems with subsuming the especially vulnerable within the policies now applied to all.
First, the medical system is being overwhelmed by those in the lower-risk group seeking its resources, limiting its capacity to direct them to those at greatest need. Second, health professionals are burdened not just with work demands, but also with family demands as schools, colleges and businesses are shuttered. Third, sending everyone home to huddle together increases mingling across generations that will expose the most vulnerable.
As the virus is already circulating widely in the United States, with many cases going undetected, this is like sending innumerable lit matches into small patches of tinder. Right now, it is harder, not easier, to keep the especially vulnerable isolated from all others — including members of their own families — who may have been exposed to the virus.
If we were to focus on the especially vulnerable, there would be resources to keep them at home, provide them with needed services and coronavirus testing, and direct our medical system to their early care. I would favor proactive rather than reactive testing in this group, and early use of the most promising anti-viral drugs. This cannot be done under current policies, as we spread our relatively few test kits across the expanse of a whole population, made all the more anxious because society has shut down.
This focus on a much smaller portion of the population would allow most of society to return to life as usual and perhaps prevent vast segments of the economy from collapsing. Healthy children could return to school and healthy adults go back to their jobs. Theaters and restaurants could reopen, though we might be wise to avoid very large social gatherings like stadium sporting events and concerts.
So long as we were protecting the truly vulnerable, a sense of calm could be restored to society. Just as important, society as a whole could develop natural herd immunity to the virus. The vast majority of people would develop mild coronavirus infections, while medical resources could focus on those who fell critically ill. Once the wider population had been exposed and, if infected, had recovered and gained natural immunity, the risk to the most vulnerable would fall dramatically.
A pivot right now from trying to protect all people to focusing on the most vulnerable remains entirely plausible. With each passing day, however, it becomes more difficult. The path we are on may well lead to uncontained viral contagion and monumental collateral damage to our society and economy. A more surgical approach is what we need.
By David L. Katz
Dr. Katz is president of True Health Initiative and the founding director of the Yale-Griffin Prevention Research Center.
Ciertamente interesante Ruindog, gracias.
Así lo intentó gestionar Boris Johnson al principio y en pocos días cambió drásticamente de opinión…
El éxito de esta estrategia (herd immunity) se basa en la habilidad que se tenga para mantener los dos grupos de población (lower and upper-risk) separados.
Los tuits que puso ayer Trump van en esta línea. Volver casi a la normalidad para semana Santa y proteger a los mayores. Ojalá funcione y no sea un error histórico.
Yo doy por hecho que cuando se vea que el efecto en la economía va a ser catastrófico, saldrá el del pelo naranja por la tele y dirá: “señores, no puede ser peor el remedio que la enfermedad, así que todo el mundo a trabajar. Trataremos a los afectados lo mejor que podamos y bla, bla, bla”
Eso pasará salvo que encuentren una cura pronto y fiable.
No los había visto hasta que los has mencionado pero parece que el articulo le ha calado hondo. Veremos 
Es que después de visto lo visto en China, Italia o España, la solución lógica es mandar de vacaciones a sus casas a todos los trabajadores mayores de 60 años previo test de coronavirus, los que den positivo a pasar las vacaciones en hoteles medicalizados. A los jubilados se les hace el mismo filtro. Por supuesto no podrán convivir en sus casas ambos grupos, trabajadores activos y mayores de 60 años, si no es posible esto los mayores de 60 años a hoteles o residencias libres de virus y bajo vigilancia.
Hay un montón de gente mayor viviendo con sus hijos y nietos, especialmente en España. La idea parece buena, pero no sé si sería factible implementarla.
En la misma linea se expreso el ministro israeli de defensa
A mi siempre me parecio la mejor idea. Cuarentena para los grupos de riesgo, ancianos, enfermos con patologias mas sensibles al virus, etc y distanciamiento social junto con mascarillas para el resto pero pudiendo hacer vida lo mas normal posible y sin parar la economia. Es el modelo de Corea del Sur y Taiwan aunque alli fueron mas rapidos a la hora de testear y aislar.
Si la teoría (como en casi todo) es muy bonita, pero la práctica…
Entonces dejamos de ver a nuestros padres hasta que haya una vacuna o un tratamiento médico? Porque sabemos que uno puede estar asintomático y contagiar… Sólo los que se contagien y tras un periodo de seguridad pueden volver a ver a sus padres??
Saludos.
Mi mujer misma tiene en Madrid una tia de 86 años en su casa “cuidada” por su nieta de 24. Me comenta que la chica no sale de casa y que le traen la comida otro nieto que a su vez “cuida” a sus padres de alrededor de 55 años y ambos con coronavirus. Espero que no pase “na” pero este virus es muy puñetero. Este panorama creo que se repite mucho en España en estos días, confío en que la higiene se extreme al máximo, sino…
Lo siento, aunque suene a conspiranoico, pero este virus es que ni pintado. Parece de diseño. Niños y jóvenes que no tienen síntomas pero pueden contagiar, curva de gravedad a partir de 60 años, velocidad de propagación record…
La sensación que yo tengo es que la mayoría de la población se niega a asumir que más tarde o más temprano va a contraer el virus.
Mantenerse alejado unos meses de la gente en situación de riesgo me parece un minúsculo precio a pagar si lo comparas con lo que estamos viviendo estos días.
A mi lo que me sorprende es todo lo que llevamos oyendo desde hace años que si Big Data, Inteligencia Artificial, Machine Learning, etc. y parece ser que la única utilidad que se le ha dado es para colarnos anuncios personalizados en internet.
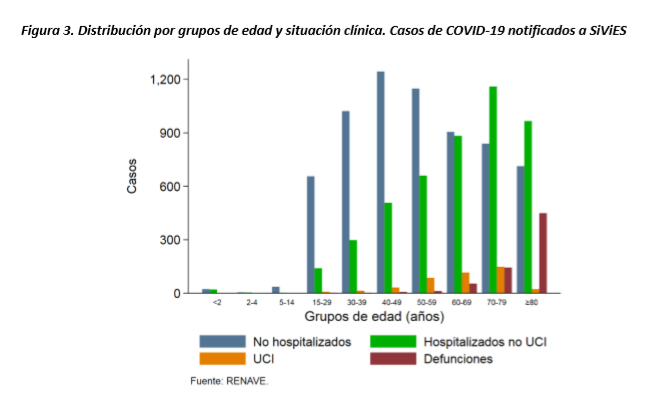
Informe nº 14. Situación de COVID-19 en España a 24 de marzo de 2020
Esta distribución por edad ya se conocía desde hace 2 meses por los casos de China. Yo he visto gráficas parecidas en los periódicos.
No me entra en la cabeza que una tecnología pueda recopilar y almacenar datos de forma que pueda aprender a conducir, pueda aprender a jugar al ajedrez y ganar a Grandes Maestros como Kasparov o sea capaz de encontrarnos un ligue justo a la vuelta de la esquina, pero no se le ha puesto ha hacer algo verdaderamente productivo analizando la distribución por edades del dichoso Coronavirus para calcular en función de la capacidad sanitaria de cada país, las medidas de cuarentena mas precisas.
Yo en esta gráfica veo que, tanto los mas vulnerables como los que mas hospitalización necesitan, son las personas de mas de 60 años. Si se evita que estas personas enfermen, se reducirá no solo la mortalidad de forma drástica, sino que también se reduciría la probabilidad de colapso del sistema sanitario a la mitad.
Gracias @ruindog
Me lo guardo para leerlo esta noche, entre el ingles y que no es un articulo precisamente corto, necesito estar tranquilo y tiempo 
¿Y no estamos sin ver a nuestros padres ahora que estamos en cuarentena?
Hace media hora me he cruzado en la calle con la profe de mis hijas. Venía de hacer la compra y se dirigía a casa de sus padres a cocinarles porque son octogenarios y viven solos 
Moraleja: cocina en casa y llévales la comida en un tupper.